
Ankylosing Spondylitis
Ankylosing Spondylitis


Back to top
What is Ankylosing Spondylitis?
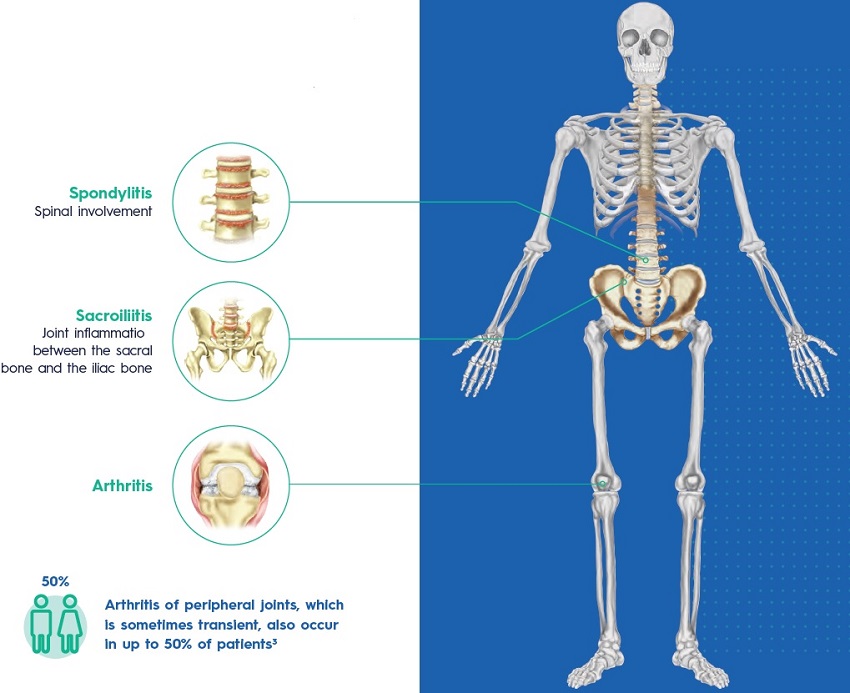
Ankylosing spondylitis (AS) is a chronic inflammatory disease that cause pain and stiffness in the back, neck and sometimes in other joints such as the hip and heels1. AS begins with inflammation around the bones in the spine or some joints, and later, it can sometimes cause the bones in the spine to fuse together, resulting in the loss of flexibility and the fusion of the spine, resembling “bamboo” with an immobile position1,2.
Back to top
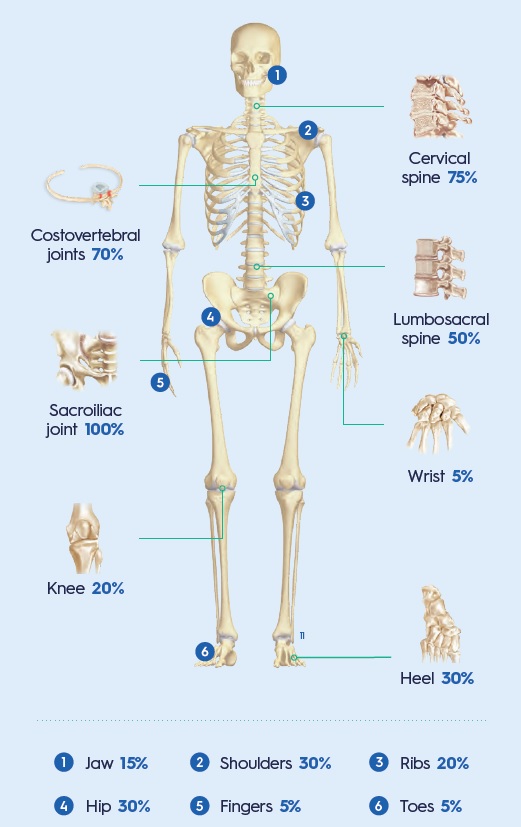
WHICH JOINTS ARE AFFECTED BY ANKYLOSING SPONDYLITIS?
Frequency of inflammation per region6
Back to top
WHAT CAUSES ANKYLOSING SPONDYLITIS?
AS is an inflammatory disease of unknown aetiology, with a higher incidence in young males2,3. As an autoimmune disease, AS develops through complex interactions between genetic background and environmental factors2.
Genetic background AS is associated with the presence of the allele HLA-B27. In fact, 90-95% of AS patients are HLA-B27 positive2.
Environmental risk factors But AS does not develop in every person who is HLA-B27 positive; thus, it is clear that environmental factors are important. Even first-degree relatives who are HLA-B27 positive do not uniformly develop the disease2.
Back to top
ASIDE FROM GENETICS, OTHER FACTORS ARE THOUGHT TO BE INVOLVED:
- Intestinal microbiome: up to 70% of patients with AS have subclinical intestinal inflammation, suggesting that the origin of the disease may be in the gut
- Infections
- Mechanical stress
- Changes in the immune system
- Gender
Back to top
WHAT ARE THE SYMPTOMS OF ANKYLOSING SPONDYLITIS?
The course of AS and its onset varies greatly from person to person, but symptoms generally start to appear in late adolescence or early adulthood (between 17 and 45 years old)5. The most common symptom is pain in the lower back and buttocks. This pain usually5:

Back to top
OTHER MANIFESTATIONS OF ANKYLOSING SPONDYLITIS
Extra-articular involvement Extraskeletal organs may also be affected by this disease. The most common extraarticular manifestations of AS include7: >50% Inflammatory bowel disease 25% to 35% Acute anterior uveitis -10% Psoriasis AS is also associated with7:
- An increased risk of cardiovascular disease.
- Pulmonary complications as diminished chest wall expansion and decreased spinal mobility predispose patients to a restrictive pulmonary pattern.
Back to top
HOW WILL MY DOCTOR DIAGNOSE MY DISEASE?
AS is diagnosed based upon the recognition of a pattern of clinical, laboratory, and imaging finding characteristic of the disease8,9.
- Physical examination9 Assessment of your flexibility and joint tenderness.
- Blood test to look at inflammatory markers8,9 C-reactive protein (CRP) or erythrocyte sedimentation rate (ESR) can be assessed in patients suspected of AS.
- Blood test which can identify if you carry the HL-B27 gene9
- X-rays9 X-rays will show if there have been any changes to your bones and joints such as extra bone growth or fusion.
- Magnetic resonance imaging (MRI) fusion9 MRI will show if there is any inflammation around your joints.
Back to top
WHAT ARE THE TREATMENT OPTIONS?
Treatment depends on your symptoms and how severe your condition is1. The goal of treatment is1:
- To relieve your symptoms
- To help you do your normal activities
- To keep your condition from causing other problems
- Patient education
- Exercises and physical therapy
- Smoking cessation
The use of a biologic agent for AS is particularly appropriate for those with high or very high disease activity, although they are effective in patients with mild to moderate symptoms as well10.
Back to top
PHARMACOLOGICAL TREATMENT
Nonsteroidal anti-inflammatory medications (NSAIDs) In many patients, NSAIDs are the only medications required as they are efficient in alleviating AS symptoms in 70-80% of patients. Biologic therapy Tumour necrosis factor (TNF)-α inhibitors. TNF inhibitors are recommended for patients with an inadequate response to initial therapy with NSAIDs. Interleukin (IL)-17 inhibitors. In patients who have contraindications to the use of TNF inhibitors, treatment with IL-17 inhibitors is recommended. Glucocorticoids Local injections of glucocorticoids into the involved joint are an option for treating arthritis as they could provide immediate symptom relief.
Back to top
WHAT CAN I DO TO MANAGE MY DISEASE?
You can reduce the chance that your conditions will cause problems if you1:
- Stop smoking (you will be less likely to have breathing problems)
- Get plenty of calcium and vitamin D (you will keep your bones from getting weak)
- Do exercise (you will prevent some of the stiffnes caused by AS)
- Use a thin pillow (sleeping on a thick pillow can cause neck problems in people with AS)
Back to top
BENEFITS OF EXERCISE
Increased flexibility The more flexible you are the easier it is to do everyday tasks. Increased range of movement The more mobility you have the easier it is to do things. Improved posture Better posture makes you feel better in yourself and reduces feelings of self consciousness. Improved sleep Exercise is physically tiring which improves sleep quality, ensuring you wake feeling refreshed. Reduction in stiffness and pain Exercise can result in less pain at night and improved sleep quality.
Back to top
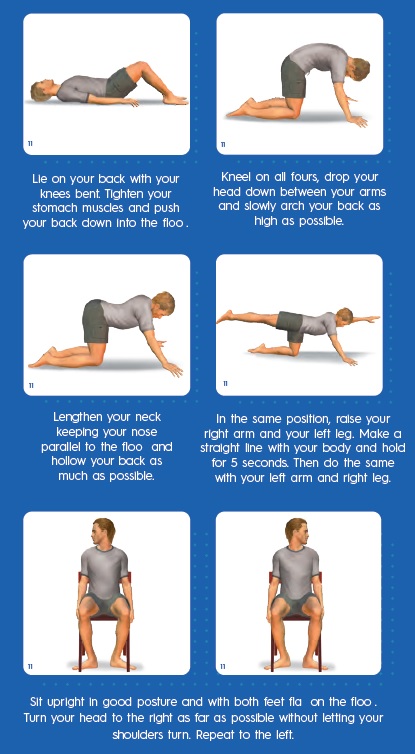
EXERCISES FOR PATIENTS WITH AS
Repeat each of the following exercises at least five times:

Medical References
- Armsby C, et al. Patient education: Ankylosing spondylitis (The Basics) [Internet]. In: UpToDate, Post, TW (Ed). [Last accessed: Dec 21, 2021]. Available at: https://www.uptodate.com/contents/ ankylosing-spondylitis-the-basics
- Zhu W, He X, Cheng K, Zhang L, Chen D, Wang X, Qiu G, Cao X, Weng X. Ankylosing spondylitis: etiology, pathogenesis, and treatments. Bone Res. 2019 Aug 5;7:22.
- Yazdany J, Manno RL. Ankylosing Spondylitis. In: Papadakis MA, McPhee SJ, Rabow MW, McQuaid KR. eds. Current Medical Diagnosis & Treatment 2022. McGraw Hill; 2022. Accessed December 21, 2021. https://accessmedicine.mhmedical.com/content. aspx?bookid=3081§ionid=258968338
- Hwang MC, Ridley L, Reveille JD. Ankylosing spondylitis risk factors: a systematic literature review. Clin Rheumatol. 2021 Aug;40(8):3079-3093.
- Spondylitis Association of America. Most common symptoms [Internet] [Last updated: Nov 15, 2021]. Available at: https://spondylitis.org/about-spondylitis/types-of-spondylitis/ankylosingspondylitis/symptoms/
- Spondylitis Association of America. Possible complications: how is a person aô€€ ected? [Internet] [Last updated: Nov 15, 2021]. Available at: https://spondylitis.org/about-spondylitis/possible-complications/
- Wenker KJ, Quint JM. Ankylosing Spondylitis. 2021 Aug 4. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2021 Jan–.
- Yu DT, van Tubergen A. Diagnosis and diô€€ erential diagnosis of axial spondyloarthritis (ankylosing spondylitis and nonradiographic axial spondyloarthritis) in adults [Internet]. UpToDate [Last updated: Mar 11, 2020]. Avaliable at: https://www.uptodate.com/contents/diagnosis-and-diô€€ erential-diagnosis-of-axialspondyloarthritis-ankylosing-spondylitis-and-nonradiographic-axialspondyloarthritis- in-adults
- National Axial Spondyloarthritis Society (NASS). Living well with axial SpA (AS) [Internet]. [Last accessed: Dec 20th, 2021]. Avaliable at: https://nass.co.uk/wp-content/uploads/2019/11/Living-well-withaxial-SpA-AS.pdf
- Yu DT, van Tubergen A. Treatment of axial spondyloarthritis (ankylosing spondylitis and nonradiographic axial spondyloarthritis) in adults [Internet]. ]. In: UpToDate, Post, TW (Ed). [Last updated: Nov 20, 2020]. Avaliable at: https://www.uptodate.com/contents/ treatment-of-axial-spondyloarthritis-ankylosing-spondylitis-andnonradiographic-axial-spondyloarthritis-in-adults
- Letter on behalf of EC Europe - 9 Feb 2022.




April 3, 2023
Content Disclaimer:
You understand and acknowledge that all users of the Dis-Chem website or app are responsible for their own medical care, treatment, and oversight. All of the content provided on the website, are for INFORMATIONAL PURPOSES ONLY and DOES NOT CONSTITUTE THE PROVIDING OF MEDICAL ADVICE and is not intended to be a substitute for independent professional medical judgment, advice, diagnosis, or treatment. The content is not intended to establish a standard of care to be followed by a user of the website. You understand and acknowledge that you should always seek the advice of your physician or other qualified health provider with any questions or concerns you may have regarding your health. You also understand and acknowledge that you should never disregard or delay seeking medical advice relating to treatment or standard of care because of information contained in or transmitted through the website. Medical information changes constantly. Therefore the information on this website or on the linked websites should not be considered current, complete or exhaustive, nor should you rely on such information to recommend a course of treatment for you or any other individual. Reliance on any information provided on this website or any linked websites is solely at your own risk.


